What is
Peyronie's disease?
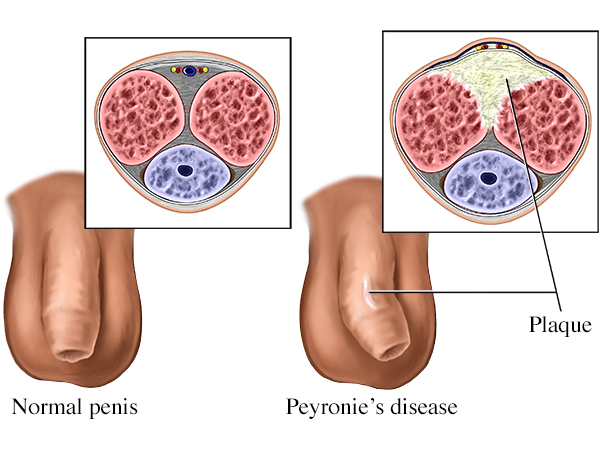
Peyronie's disease is a condition where scar tissue (plaque) forms under the skin of the penis, causing the penis to curve, bend, shorten, or develop indentations during erection. The plaque most commonly forms in the tunica albuginea — the fibrous covering of the erectile bodies. As the plaque is non-stretchy while surrounding tissue is, the erect penis bends toward the plaque side.
The cause is generally believed to be micro-trauma during intercourse that doesn't heal normally. In susceptible men, the body's healing response over-produces scar tissue rather than smoothly remodelling. Genetic predisposition, connective tissue disorders, diabetes, and ageing all increase the risk of this abnormal healing.
Peyronie's affects an estimated 6–9% of adult men, though the true prevalence is likely higher because many men don't seek help. It's most common in men between 40 and 70 but can occur at any age. The course is typically: a starting period of pain and curvature development (acute phase), followed by stabilisation (chronic phase) where curvature persists but pain resolves.
Acute and chronic —
different treatments.
Acute (Active) Phase
The plaque is actively forming. Pain may be present during erections. Curvature is developing or worsening. The condition is unstable — changes month to month. Goal of treatment: limit progression and reduce inflammation.
Chronic (Stable) Phase
The plaque has matured. Pain has usually resolved. Curvature has stabilised. No further progression expected. Goal of treatment: correct established deformity if it's interfering with function.
How We Confirm Stability
Curvature stable for at least 6 months. No pain. Plaque size unchanged. Often documented with serial photographs and measurements. Surgery considered only in stable phase.
What Happens Without Treatment
About 13% of men show spontaneous improvement. About 40% remain stable. About 47% worsen during the acute phase. Treatment in the acute phase aims to maximise the proportion who don't worsen.
Why Peyronie's
develops.
The exact cause isn't fully understood, but Peyronie's is generally believed to result from abnormal healing after micro-injury to the penis. Risk factors include:
- Repeated micro-trauma during intercourse — particularly with vigorous activity
- Acute injury — penile fracture, sports injury, vehicular trauma
- Genetic predisposition — family history of Peyronie's or Dupuytren's contracture (a hand condition involving similar abnormal scar formation)
- Connective tissue disorders — Dupuytren's contracture, plantar fasciitis
- Diabetes — significantly increases risk
- Hypertension and cardiovascular disease — increase risk
- Erectile dysfunction — frequently coexists with Peyronie's, in either direction
- Smoking — increases risk
- Pelvic radiation or surgery — particularly after prostatectomy
- Ageing — most cases occur between 40 and 70
- Hypogonadism — low testosterone may contribute
- Beta-blocker use — uncertain but suggested association
How Peyronie's
presents.
Symptoms vary depending on phase and severity:
- Curvature of the penis on erection — upward, downward, sideways, or combinations. May be subtle or severe.
- Pain during erection — particularly in the acute phase. Usually settles by 12–18 months even without treatment.
- A palpable lump or hardened area — the plaque is felt as a firm nodule or band beneath the skin of the penis
- Shortening of the penis — both erect and flaccid length
- Hour-glass deformity — narrowing or indentation of the penis at the level of the plaque
- Hinge effect — buckling of the penis at the affected area during intercourse
- Difficulty with intercourse — mechanical, painful, or impossible depending on severity
- Erectile dysfunction — develops in 30–50% of Peyronie's patients, either from associated vascular issues or psychological factors
- Psychological distress, relationship strain, depression — common and significant. The emotional impact is often as important as the physical.
Examination plus
objective measurement.
Peyronie's diagnosis is largely clinical. Key elements of the workup:
- Detailed history — duration of symptoms, pain, progression, sexual function, prior trauma, family history, comorbidities
- Examination of flaccid penis — palpation identifies plaque location, size, and consistency
- Examination of erect penis — objective measurement of curvature direction and angle. This is critical for treatment planning. Done either with a pharmacologically-induced erection in clinic, or by reviewing patient-provided photographs at home (a more practical option many patients prefer).
- Penile ultrasound — confirms plaque, measures size, assesses calcification (a marker of chronic stable plaque), evaluates vascular flow.
- Assessment of erectile function — IIEF-5 questionnaire and history. Erectile dysfunction coexists in 30–50% of Peyronie's patients and changes treatment planning.
- Photographic documentation — for tracking progression over time. Patient-taken photos at home are confidential and clinically useful.
Phase-appropriate
options.
Treatment in the acute (active) phase:
- Observation — for mild disease, monitoring is reasonable. About 13% improve spontaneously.
- Oral medications — pentoxifylline, vitamin E, colchicine. Evidence modest but used in selected cases.
- Penile traction therapy — daily traction device used over months. Modest evidence for reducing curvature and preserving length. Particularly useful in the acute phase.
- Vacuum erection devices — daily use to maintain elasticity and prevent shortening.
- Pain management — anti-inflammatories or simple analgesia during painful erections.
- Treatment of contributing factors — diabetes control, smoking cessation, treatment of ED with PDE5 inhibitors.
Treatment in the chronic (stable) phase:
- Continued traction therapy — for selected stable cases
- Intralesional injections — collagenase clostridium histolyticum (where available), verapamil, interferon. Modest effectiveness. Often multiple cycles required. Coordinated with specialised centres where available.
- Surgery — definitive correction of significant stable deformity. Several techniques (covered below).
- Penile prosthesis — for patients with both Peyronie's and significant erectile dysfunction. Solves both problems.
When surgery is
the right answer.
Surgery is considered when:
- The disease is stable (chronic phase, at least 6 months without progression)
- Curvature is severe enough to prevent intercourse
- Pain has resolved
- Other conservative measures have failed or aren't appropriate
- The patient understands the goals and limitations
Three main surgical approaches:
- Plication surgery (Nesbit / Lue procedure) — the longer convex side of the curved penis is shortened with sutures to match the shorter concave side. Straightens the penis but results in some shortening. Simpler procedure, lower complication rate. Good for curvatures under 60 degrees with good erectile function.
- Plaque incision and grafting — the plaque is incised, and a graft (vein, bovine pericardium, or other material) is placed to lengthen the shortened side. Preserves penile length but more complex, with somewhat higher risk of erectile dysfunction. Better for severe curvature, hour-glass deformity, or where length preservation matters most.
- Penile prosthesis insertion — for patients with Peyronie's plus significant ED. The implant corrects both. Often combined with simultaneous manual modelling or grafting if curvature persists.
What to expect after surgery:
- Hospital stay 1–2 nights
- Catheter for 1–2 days
- Avoid sexual activity for 6–8 weeks
- Light activity from 1 week, gradual return to full activities
- Most patients see straightened erections after healing
- Some shortening typical with plication; minimal with grafting
Considered care
for a sensitive
diagnosis.
Confidential evaluation
Private consultation. Photographic documentation reviewed and not retained. Discreet billing where requested. The diagnosis is yours alone.
Phase-appropriate treatment
We don't operate during the acute phase. We treat medically while the condition stabilises, then assess for surgery if needed.
Surgical capability
Plication and grafting techniques performed in-house. Penile prosthesis insertion coordinated with partner centres where appropriate.
Honest expectations
We tell you realistic outcomes — no procedure restores everything to pre-Peyronie's baseline. Plication shortens; grafting can affect erection. We discuss trade-offs openly.
Pricing for Peyronie's
care.
| Service | Starting from |
|---|---|
| Confidential consultation | ₹ [____] |
| Penile ultrasound | from ₹ [____] |
| Penile Doppler with pharmacological erection | from ₹ [____] |
| Traction therapy device | from ₹ [____] |
| Oral therapy (per month) | from ₹ [____] |
| Intralesional injection (per cycle) | from ₹ [____] |
| Plication surgery (Nesbit / Lue) | from ₹ [____] |
| Plaque incision with grafting | from ₹ [____] |
Surgery sometimes covered. OPD often self-pay.
Surgical correction of Peyronie's may be covered when functional impairment is documented. OPD investigation and conservative treatment usually self-pay. We discuss costs upfront and accommodate patients preferring private payment for confidentiality.
Peyronie's disease —
your questions.
Spontaneous improvement occurs in about 13% of patients. Stabilisation without further progression is more common. Significant worsening also occurs in about 47% of untreated patients. Early evaluation gives the best chance of preserved function.
Generally not during the acute phase. Surgery is considered when the condition has been stable for at least 6 months, the curvature is severe enough to interfere with intercourse, and conservative options have failed or aren't appropriate. Rushing into surgery during the active phase risks recurrence.
Surgery aims to straighten the penis enough for successful intercourse, not to restore exactly pre-Peyronie's anatomy. Plication shortens the penis. Grafting may affect erectile function. We discuss realistic expectations honestly before any surgical decision.
Peyronie's doesn't directly affect sperm production. Indirectly, severe curvature can make intercourse mechanically difficult or impossible, which affects natural conception. With treatment that restores functional intercourse, fertility is generally not affected.
In most patients yes — pain typically resolves by 12–18 months of disease onset, even without treatment. Pain rarely persists in the chronic phase. Pain management during the acute phase makes the wait more comfortable.
Yes. PDE5 inhibitors (sildenafil, tadalafil) often help. For severe ED with Peyronie's, penile prosthesis insertion solves both problems simultaneously.
Yes — absolutely. Private consultation, confidential records, discreet billing options. Family members and employers are not informed.
Yes — many men prefer this. Photos sent to +91 9509370455 are reviewed confidentially and help us advise whether you need an urgent appointment or routine. Photos are not retained on devices.