Stage at diagnosis
changes everything.
Penile cancer is one of the clearest examples in medicine where when you present matters as much as what you present with. A small lesion confined to the foreskin or surface of the penis, identified within weeks of appearing, can often be cured by a minor local procedure — sometimes a circumcision alone is enough. The same cancer, allowed to grow for six months because the patient was too embarrassed to come in, may need partial removal of the penis, lymph node surgery, and chemotherapy.
The reasons most men wait too long are universal: embarrassment, hope it will go away, fear of what the diagnosis might be, lack of awareness that penile cancer exists at all. None of these change the underlying biology. The lesion grows, lymph nodes get involved, and the treatment escalates.
If you have noticed something on your penis — a lump, a sore that isn't healing, a thickened patch of skin, a change in colour, bleeding, or a smell — bring it in. The cost of a 20-minute consultation is meaningless against the cost of months of worry, or worse, of late diagnosis. You can WhatsApp a photo first if that feels easier — we review confidentially and tell you whether it warrants an urgent visit.
What is
penile cancer?
Penile cancer is a malignant tumour that develops on the penis — most commonly the glans (head), the foreskin, or the shaft skin. Over 95% of penile cancers are squamous cell carcinoma, arising from the surface skin cells. Less common types include basal cell carcinoma, melanoma, and sarcomas.
It is uncommon in countries where circumcision is widespread, more common in countries where it isn't. India sits in the higher-incidence range, with a rate of roughly 0.7 to 3 per 100,000 men depending on the region. Most cases occur in men over 50, but younger men are affected too.
Penile cancer often develops from precancerous skin changes — chronic inflammation, persistent infection, untreated lichen sclerosus, or HPV-related lesions. These changes can sit on the skin for years before progressing to invasive cancer. Recognising and treating precancerous changes prevents a substantial proportion of penile cancers.
What raises
the risk.
Penile cancer doesn't occur randomly. Several well-established risk factors raise the chance of developing it:
- Phimosis — a tight foreskin that cannot be retracted is one of the strongest risk factors. Chronic inflammation under an unretractable foreskin sets the stage for malignant change over years.
- Poor genital hygiene — the inability to retract and clean the foreskin allows smegma to accumulate, causing chronic irritation.
- HPV infection — particularly high-risk strains (16, 18). HPV is identifiable in about 30–50% of penile cancers.
- Chronic balanitis — long-standing inflammation of the glans or foreskin, especially when untreated for years.
- Lichen sclerosus (BXO) — an autoimmune-type skin condition affecting the foreskin and glans. Long-standing untreated BXO is a recognised precancerous condition.
- Smoking — significantly increases risk, particularly in combination with HPV.
- Immunosuppression — HIV, transplant medications, chemotherapy.
- Multiple sexual partners and history of STIs — partly through increased HPV exposure.
- Age over 50 — incidence rises with age.
- PUVA therapy — historical UV-based skin treatments raised genital cancer risk.
What to look for —
and when to come in.
The earliest signs of penile cancer can be subtle. Look for changes in the skin of the glans, the foreskin, or the shaft:
- A new lump, growth, or thickened patch — particularly on the glans or under the foreskin
- An ulcer or sore that doesn't heal within 2–3 weeks
- Persistent change in skin colour — a white, red, or pigmented patch
- Bleeding from the skin or under the foreskin
- A foul-smelling discharge, especially from under a phimotic foreskin
- Velvety red patches on the glans (suggestive of carcinoma in situ)
- A wart-like growth that doesn't respond to typical wart treatment
- Painless lumps in the groin — possibly indicating spread to lymph nodes
- Persistent irritation or rash not responding to topical creams within a few weeks
Pain is often not an early feature — many penile cancers are painless until they're locally advanced. The absence of pain should not reassure you. A painless persistent change is exactly what to flag.
If you have phimosis and have never been able to fully retract your foreskin to examine the glans — see us specifically for that. A lesion can hide under a phimotic foreskin for months, undetected, simply because the foreskin cannot be pulled back to look. Circumcision in this context is both diagnostic and therapeutic.
What the workup
looks like.
Diagnosing penile cancer is straightforward in most cases — examination plus a biopsy of the lesion confirms or excludes malignancy. The work is in staging — figuring out whether it has spread.
Standard workup:
- Examination — careful inspection of the entire penis, the inguinal lymph nodes in both groins, and the scrotum. A tight foreskin may need to be retracted under anaesthesia (or circumcised) to see the underlying glans.
- Biopsy — a small piece of tissue taken from the lesion under local anaesthesia, sent for histology. Confirms the diagnosis, grade, and depth of invasion.
- HPV testing — sometimes done on the biopsy specimen.
- Lymph node assessment — palpation of the groins, ultrasound of the inguinal regions. If any nodes are suspicious, fine-needle aspiration cytology (FNAC) or biopsy.
- MRI of the penis — for larger lesions, to assess local extent and corporal invasion before surgery.
- CT chest/abdomen/pelvis — for staging in higher-risk cases, looking for distant spread.
- PET-CT — selectively, in advanced disease.
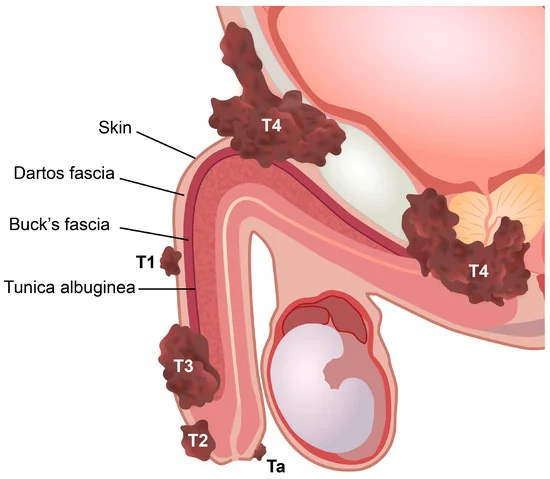
Stage determines
treatment.
Carcinoma in situ
Confined to the surface skin layer. Has not invaded deeper tissues. Often treated with topical chemotherapy or local excision. Excellent outcomes.
Early invasive
Invades the layer below the skin but no deeper. Treatment typically organ-preserving local surgery or laser. Lymph nodes may need evaluation.
Corporal invasion
Invades the corpus spongiosum or corpus cavernosum (the erectile bodies). Larger surgery often needed. Lymph node evaluation essential.
Locally advanced
Invades the urethra, prostate, or other adjacent structures. Multi-modality treatment combining surgery, lymph node dissection, and chemotherapy.
In addition to the T (tumour) stage, the N (lymph node) and M (metastasis) status guides treatment:
- N0 — no lymph node involvement. Best prognosis.
- N1–N3 — increasingly involved lymph nodes. Treatment escalates.
- M0/M1 — distant spread absent or present.
Survival outcomes vary dramatically by stage: 85%+ 5-year survival for early-stage disease, dropping into single digits for advanced metastatic disease. Early diagnosis is the single biggest factor in outcome.
From organ preservation
to multi-modality care.
The first principle of modern penile cancer treatment is organ preservation wherever oncologically safe. Outdated approaches removed more tissue than necessary out of excess caution. Modern surgery aims to remove the cancer fully while preserving as much function and form as possible.
For early-stage disease (Ta, Tis, T1, small T2):
- Topical chemotherapy (5-fluorouracil, imiquimod) — for carcinoma in situ. Cream applied to the lesion for weeks. Avoids surgery in selected cases.
- Laser therapy — laser ablation of superficial lesions. Preserves the underlying tissue.
- Wide local excision — surgical removal of the lesion with a margin of healthy tissue.
- Circumcision — sometimes curative on its own, when the cancer is confined to the foreskin.
- Glansectomy — removal of part or all of the glans with reconstruction. Preserves penile length and most sexual function.
- Mohs micrographic surgery — for selected lesions, tissue removed in layers with immediate microscopic examination.
For more advanced disease:
- Partial penectomy — removal of the distal portion of the penis. Sexual function can be preserved depending on residual length. Standing urination preserved in most cases.
- Total penectomy with perineal urethrostomy — reserved for advanced cancer invading the body of the penis. Urination is redirected through an opening between the legs.
- Inguinal lymph node dissection — removal of groin lymph nodes when involved or at high risk. Modern modified dissections reduce side effects.
- Chemotherapy — for lymph node-positive disease or distant metastasis. Coordinated with medical oncology.
- Radiotherapy — for selected primary tumours where organ preservation is desired, or for nodal disease.
What actually
reduces risk.
Treat Phimosis
Phimosis that has been present for years is one of the strongest risk factors. Adult circumcision dramatically reduces penile cancer risk. Done as ZSR circumcision at the clinic — stitchless, day-care.
Genital Hygiene
Daily retraction and washing of the foreskin (if anatomically possible). Removal of accumulated smegma. Simple, free, effective.
HPV Vaccination
HPV vaccination in adolescents — both boys and girls — reduces the incidence of HPV-related cancers including penile cancer. Most effective when given before sexual activity begins.
Stop Smoking
Smoking is an independent risk factor for penile cancer. Cessation reduces future risk, particularly when combined with addressing other risk factors.
Address Precancerous Conditions
Lichen sclerosus (BXO), chronic balanitis, persistent skin patches — all should be diagnosed and treated rather than ignored. Many penile cancers develop from these conditions over years.
Self-Examination
Brief monthly self-examination during washing — looking for new lumps, sores, or skin changes. Anything new and persistent over 2–3 weeks warrants evaluation.
Dignified care
for a sensitive
diagnosis.
Confidential evaluation
Private consultation, discreet billing where requested. The diagnosis is yours alone — not your family's, not your office's. We protect this strictly.
WhatsApp photo screening
If you're not sure whether what you're seeing warrants a visit, send a photo over WhatsApp. We review confidentially and tell you honestly whether you need to come in.
Organ-preserving surgery
We default to the least-mutilating procedure that achieves oncological control. Laser, local excision, glansectomy — rather than reflexive radical surgery.
Multi-disciplinary coordination
Advanced cases need coordination with medical oncology, radiation oncology, and reconstructive surgery. We arrange this, not just refer.
Pricing for penile
cancer care.
| Service | Starting from |
|---|---|
| Confidential consultation | ₹ [____] |
| Biopsy of suspicious lesion | from ₹ [____] |
| MRI penis (staging) | from ₹ [____] |
| Ultrasound inguinal nodes | from ₹ [____] |
| CT chest/abdomen/pelvis (full staging) | from ₹ [____] |
| Wide local excision / laser ablation | from ₹ [____] |
| Glansectomy with reconstruction | from ₹ [____] |
| Partial penectomy | from ₹ [____] |
| Inguinal lymph node dissection | from ₹ [____] |
Cashless cancer surgery with all major insurers.
Cancer surgery, biopsy, staging investigations, and reconstruction are covered by all major Indian insurers. For patients who prefer privacy from family or employer, we can bill in ways that avoid disclosure of specific diagnosis where possible. We handle pre-authorisation.
Penile cancer —
your questions.
Most penile lumps and skin changes are benign — warts, cysts, balanitis, lichen sclerosus, pearly penile papules. But anything new, persistent over 2–3 weeks, ulcerating, bleeding, or growing warrants evaluation. The cost of getting it checked is much less than the cost of months of worry. You can WhatsApp a photo first if that feels easier.
Yes. Medical confidentiality is absolute. The consultation room is private, records are confidential, and family members are not informed without your written consent. For insurance claims where privacy is a concern, we can use diagnostic coding that doesn't disclose specifics where possible.
Almost never for early-stage disease. Modern treatment defaults to organ-preserving approaches — topical chemotherapy, laser ablation, wide local excision, glansectomy with reconstruction. Total penectomy is reserved for locally advanced disease where it's the only oncologically safe option. Early diagnosis is the key to preserving the penis.
Depends on the extent of treatment. Topical and superficial treatments often leave function intact. Glansectomy with reconstruction preserves erectile function and most sensation. Partial penectomy preserves erectile function but with shorter penile length. Total penectomy ends penetrative sexual function — but is now rare with early diagnosis. We discuss honestly before any treatment.
Sexual activity itself is not a direct cause, but some risk factors — particularly HPV infection — are sexually transmitted. Most penile cancers, however, occur in older men with long-standing phimosis or chronic skin conditions, where sexual activity is not the main driver.
Adult circumcision is recommended if you have phimosis (tight foreskin), recurrent balanitis, or lichen sclerosus. In these situations it dramatically reduces penile cancer risk. Circumcision in men without any risk factors is a personal choice — preventive value exists but is modest in low-risk populations.
Typically 7–10 days. We schedule a follow-up consultation to discuss the result in person — never deliver a cancer diagnosis over the phone. If urgent imaging is also needed, we coordinate this with the biopsy result review.
Yes — all major Indian health insurers cover cancer surgery, biopsy, staging investigations, and reconstruction. CGHS and ECHS panels also covered. We handle pre-authorisation and can support discreet billing where privacy is a particular concern.
Yes — for visible concerns, WhatsApp a photo to +91 9509370455. We review confidentially and tell you honestly whether you need an urgent appointment, a routine one, or whether the concern is benign. Photos remain confidential.