What is
a hydrocele?
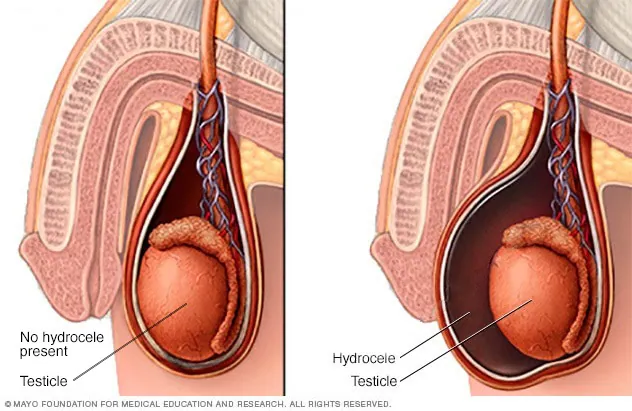
A hydrocele is an accumulation of fluid in the tunica vaginalis — a thin sac that surrounds the testicle. It produces a painless, soft scrotal swelling on one or sometimes both sides. The fluid is clear and yellow; the testicle floats inside it.
Hydroceles can occur at any age. In infants, they are often present at birth and typically resolve on their own by age one or two. In adults, hydroceles usually develop slowly over months to years and gradually enlarge. Some remain small and untroubling for decades. Others grow large enough to interfere with sitting, walking, sexual function, or simply confidence.
The key reassurance: hydroceles are almost always benign. They do not turn into cancer. They do not affect fertility in most cases. The decision to operate is based on symptoms and size, not on any medical urgency.
Four clinical
presentations.
Idiopathic Hydrocele
Develops without identifiable cause in adult men. Slowly enlarging, painless, one-sided typically. The standard hydrocele.
Congenital Hydrocele
Present from birth, due to incomplete closure of the processus vaginalis (the channel between abdomen and scrotum). Usually resolves by age 1–2. Surgery only if persistent or symptomatic.
Communicating Hydrocele
Has connection to the abdominal cavity — fluid moves between abdomen and scrotum. Hydrocele changes size during the day. Often associated with hernia.
Secondary Hydrocele
Develops after trauma, surgery, infection (epididymitis, orchitis), or in association with testicular tumour. Important to identify the underlying cause before treatment.
Why hydroceles
develop.
In adults, hydroceles often appear without a clear cause. The mechanism involves an imbalance between fluid production by the tunica vaginalis and fluid absorption — but the trigger for this imbalance is frequently not identifiable. Known causes and associations include:
- Idiopathic (most common) — no identifiable cause
- Past trauma — sometimes scrotal injury years earlier triggers fluid accumulation
- Past or current infection — epididymitis, orchitis, tuberculosis
- Filariasis — historically a major cause in some regions of India, though incidence has dropped significantly
- Underlying testicular tumour — important to exclude in any new hydrocele in an adult man
- Post-surgical — after groin surgery, varicocele repair, undescended testis surgery
- Congenital — patent processus vaginalis in infants and young children
How hydroceles
present.
Hydroceles are typically painless. The presenting features are usually mechanical and cosmetic:
- Painless scrotal swelling — gradually enlarging over months
- Heaviness or dragging sensation — particularly with larger hydroceles
- Discomfort with sitting, walking, or exercise — when the hydrocele becomes large
- Difficulty finding comfortable underwear or trousers
- Embarrassment or self-consciousness — particularly during intimacy
- Difficulty with sexual function — large hydroceles can interfere mechanically
- Skin changes — with very large long-standing hydroceles, the scrotal skin can stretch and become thin
Features that should prompt urgent evaluation:
- Pain in the hydrocele or testicle (suggests infection, torsion, or other pathology)
- Sudden onset
- Red, hot scrotum (suggests infection)
- Fever
- Inability to feel the testicle through the hydrocele (warrants ultrasound)
Two simple tests
confirm everything.
Hydrocele diagnosis is straightforward and usually completed in a single visit:
- Examination — a hydrocele feels soft, smooth, and fluid-filled. The classic finding is transillumination — shining a torch through the scrotum reveals the fluid as a glowing translucent area, while a solid lump (like a tumour) would not transilluminate.
- Scrotal ultrasound — confirms the diagnosis, measures the hydrocele, and most importantly, visualises the testicle to ensure it is normal. Essential before any treatment decision.
- Blood tests — not routinely required, but tumour markers (AFP, beta-hCG, LDH) may be checked if there's any doubt about the testicle.
The ultrasound is the single most important investigation. It confirms the hydrocele is benign, rules out a testicular tumour as the underlying cause, and provides a measurement that helps in surgical planning.
Three options,
matched to severity.
Observation
Small hydroceles that aren't causing symptoms can simply be monitored. Annual examination. No treatment unless they grow or become symptomatic.
Open Hydrocelectomy
The standard surgical treatment. A small scrotal incision, the hydrocele sac drained and either excised or folded back (Jaboulay's plication). Day-care surgery. Very low recurrence rate. The standard of care for symptomatic hydroceles.
Aspiration + Sclerotherapy
The fluid is drained with a needle, and a sclerosing agent injected to discourage refilling. Less invasive, but recurrence rates are 30–50%. Reserved for patients unfit for surgery or where surgery is declined.
Why surgery is preferred over aspiration: Aspiration alone is almost universally followed by re-accumulation. Even with sclerotherapy, recurrence is high. Surgery removes the underlying problem (the abnormal sac) rather than just removing its content. For symptomatic hydroceles, surgery is generally the right answer.
What to expect
after surgery.
- Day of surgery — done under spinal or general anaesthesia. About 60–90 minutes. Most patients discharged same day after a few hours of observation.
- Days 1–3 — mild to moderate scrotal swelling, soreness. Scrotal support recommended. Simple analgesia (paracetamol, sometimes a short course of anti-inflammatories). Cold compresses help.
- Days 4–7 — swelling settles. Wound dressing changed. Most desk workers ready to return.
- Week 2 — wound largely healed. Avoid gym, cycling, and heavy lifting.
- Week 3–4 — full return to all activities including sexual activity. Final wound check.
- Month 3 — final follow-up. Excellent outcomes in over 98% of patients.
Complications are uncommon but can include haematoma (bleeding into the scrotum), infection, or recurrence. We discuss these openly before surgery and monitor for them after.
Quick, definitive,
day-care surgery.
Day-care protocol
Walk in morning, walk out evening. No overnight stay needed for most patients. Designed for the working man's schedule.
Modern technique
Small scrotal incision, sac excision or plication based on size and tissue quality. Excellent cosmetic outcome.
Ultrasound always done
Pre-op ultrasound confirms the underlying testicle is normal. We don't operate on hydrocele without confirming it's not concealing something else.
Bilateral in single setting
For bilateral hydroceles, both sides done in the same anaesthetic. One recovery period, one cost setup, one return to normal.
Pricing for hydrocele
treatment.
| Service | Starting from |
|---|---|
| Consultation + examination | ₹ [____] |
| Scrotal ultrasound | from ₹ [____] |
| Hydrocelectomy (unilateral, day-care) | from ₹ [____] |
| Hydrocelectomy (bilateral, single setting) | from ₹ [____] |
| Aspiration + sclerotherapy | from ₹ [____] |
| Post-op review | from ₹ [____] |
Hydrocelectomy is covered by all major insurers.
Hydrocelectomy is a covered surgical procedure under all major Indian health insurance policies with cashless TPA support. We handle pre-authorisation. Personalised quotes available on consultation.
Hydrocele —
your questions.
In infants and young children — often yes, by age 1–2. In adults — generally no. Adult hydroceles tend to persist or slowly enlarge over time. Spontaneous resolution in adults is rare.
In most cases no. Hydroceles around the testicle don't typically affect sperm production. Very large or long-standing hydroceles may have some impact through pressure or temperature effects, but this is uncommon. If you're concerned about fertility, a semen analysis can be done.
Done under spinal or general anaesthesia, so no pain during. Mild to moderate scrotal soreness for 5–7 days afterwards, controlled with simple analgesia. Most patients describe it as manageable.
A small scrotal incision (3–4 cm) is made. It heals to a fine line that fades significantly over months. Cosmetic outcome is generally excellent.
Recurrence after proper surgical hydrocelectomy is under 2%. After aspiration alone, recurrence is 80%+. After aspiration with sclerotherapy, 30–50%. Surgery is definitively curative in the vast majority of cases.
Desk work: 5–7 days. Physical work or gym: 3–4 weeks. Sexual activity: 2–3 weeks. Driving: 3–5 days. Most patients are comfortable with light activities within a week.
Aspiration alone has very high recurrence (often within weeks). Sclerotherapy reduces recurrence but is still inferior to surgery. We generally recommend surgery for symptomatic hydroceles. Aspiration is reserved for patients unfit for anaesthesia or who decline surgery.
Yes — hydrocelectomy is covered by all major Indian health insurers with cashless TPA support. We handle pre-authorisation paperwork.