Sudden severe one-sided testicular pain — particularly in a younger man — is testicular torsion until proven otherwise.
Don't wait. Don't observe. Don't apply hot or cold packs. Testicular torsion is a surgical emergency. The window to save the testicle is approximately 6 hours from onset. Call +91 9509370455 immediately or go straight to the nearest emergency room.
📞 Call Emergency LineSudden pain
has limited possibilities.
Pain that starts suddenly — over minutes to a few hours — and is severe, has a specific differential diagnosis. The first job is excluding the surgical emergencies.
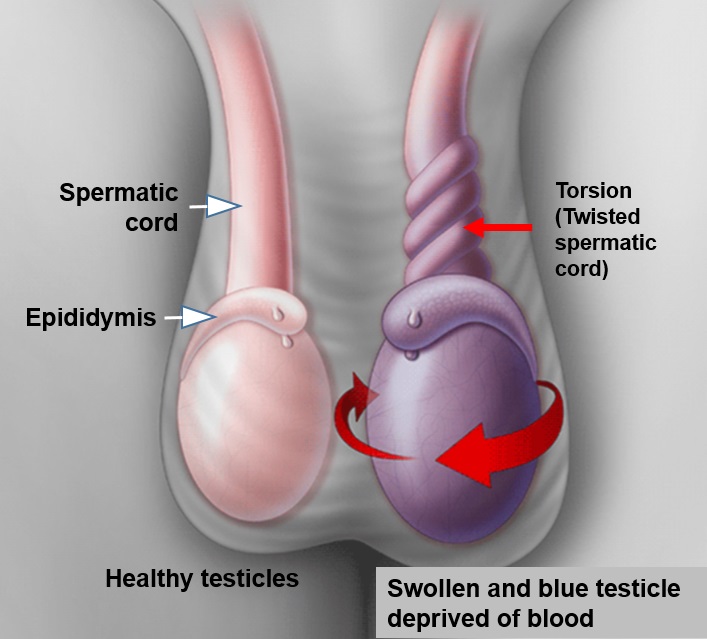
Testicular torsion — the absolute emergency
The spermatic cord twists, cutting off blood supply to the testicle. Most common in adolescents and young men but possible at any age. Sudden severe one-sided pain, often with nausea and vomiting. The testicle may sit higher than normal and may be horizontal rather than vertical. Every hour matters. 90%+ salvage rate if operated within 6 hours; under 50% after 12 hours. If torsion is suspected, the patient goes straight to theatre — sometimes without waiting for ultrasound confirmation.
Acute epididymo-orchitis — infection of the testicle and/or epididymis
Develops over hours to days rather than minutes. Pain associated with swelling, often with fever, sometimes with urinary symptoms (burning, frequency). May be sexually transmitted (chlamydia, gonorrhoea) in younger men or from bladder/prostate infection in older men. Treated with antibiotics, rest, scrotal support, and anti-inflammatories. Usually settles over 1–2 weeks.
Testicular trauma
Sports injury, accident, deliberate trauma. Most cases resolve with rest and supportive care. Severe trauma can cause testicular rupture or haematoma — requires urgent ultrasound and sometimes surgery.
Strangulated inguinal hernia
A hernia that has slipped into the scrotum and gotten trapped. Causes severe groin and scrotal pain. Surgical emergency.
Torsion of testicular appendix
A small embryological remnant on the testicle twists. Severe pain similar to torsion but without complete loss of blood supply. Usually settles with rest and analgesia. Diagnosed when ultrasound shows normal testicular blood flow.
When pain has been
present for months.
Varicocele
Dragging or aching pain, worse with standing, end-of-day, hot weather, or exercise. Relieved by lying down. Diagnosed on examination and Doppler ultrasound. More on varicocele →
Chronic Epididymitis
Long-standing low-grade inflammation of the epididymis. Aching pain, sometimes following an acute episode. Diagnosed by examination and ultrasound. Treatment varies — sometimes antibiotics, sometimes anti-inflammatories, occasionally surgery.
Spermatocele or Cyst
Fluid-filled cyst on the epididymis. Usually painless but large ones can cause discomfort. Diagnosed on ultrasound. Surgery only if symptomatic.
Testicular Tumour
Most testicular cancers are painless lumps, but a minority present with pain. Any new persistent pain warrants ultrasound to exclude this.
Referred Pain
Pain from elsewhere felt in the testicle — ureteric stones, hip pathology, inguinal hernia, lumbar nerve compression. The testicle examination is normal; the cause is elsewhere.
Post-Vasectomy Pain Syndrome
Chronic testicular or scrotal pain after vasectomy. Affects a small percentage of vasectomy patients. Treatment includes anti-inflammatories, sometimes vasectomy reversal.
Chronic Scrotal Pain Syndrome
Long-standing pain with no clear structural cause despite full workup. Treatment is multimodal — pain medications, nerve blocks, physiotherapy, sometimes psychological support.
Hydrocele
Usually painless, but large ones can cause heaviness and discomfort. Diagnosed on examination and transillumination. More on hydrocele →
From history
to imaging.
The clinical approach depends entirely on whether the pain is acute or chronic. For both, the standard evaluation includes:
- Detailed history — onset (sudden vs gradual), duration, character (sharp, dull, dragging), radiation, aggravating/relieving factors, urinary symptoms, sexual history, trauma, fever
- Examination — testicular size, position, tenderness, presence of masses, Prehn's sign, cremasteric reflex, inguinal examination for hernia, abdominal examination for referred pain
- Scrotal Doppler ultrasound — single most useful investigation. Confirms or excludes torsion (no blood flow vs normal), identifies varicocele, hydrocele, masses, abscess, hernia
- Urine analysis & culture — for suspected infection
- STI screen — for younger patients with epididymitis
- Tumour markers — if testicular mass identified (AFP, beta-hCG, LDH)
- MRI — selectively for complex chronic pain or post-trauma evaluation
- Pain diary — for chronic pain, sometimes helpful for identifying patterns
For acute pain suggestive of torsion, the workup is compressed dramatically. If clinical suspicion is high, the patient goes to theatre without waiting for imaging. Time saved is testicle saved.
Matched to
cause.
For testicular torsion: emergency surgical exploration. The twist is reversed, the testicle assessed for viability, and both testicles fixed in place (orchidopexy) to prevent future torsion. If the testicle is non-viable, removal (orchidectomy) is necessary.
For acute epididymo-orchitis: antibiotics for 10–14 days (longer for severe cases), pain control, anti-inflammatories, scrotal support, rest. Most resolve within 2–4 weeks. Partner treatment for STI-related cases.
For varicocele-related pain: conservative measures first (scrotal support, NSAIDs, lifestyle adjustments). Microsurgical varicocelectomy if pain persists and is clearly attributable to the varicocele.
For chronic epididymitis: trial of long course antibiotics, anti-inflammatories. Failed cases may consider epididymectomy.
For symptomatic spermatocele or cyst: surgical removal.
For referred pain: treat the underlying cause — stone removal, hernia repair, lumbar issue management.
For post-vasectomy pain syndrome: initial conservative management with anti-inflammatories and nerve blocks. Refractory cases may require vasectomy reversal.
When no structural
cause is found.
In a meaningful proportion of patients with chronic testicular pain, full workup finds no clear structural cause. This is chronic scrotal pain syndrome — pain that is real but without an identifiable target for surgical intervention.
Treatment for chronic scrotal pain syndrome is typically multimodal:
- Anti-inflammatory medications — short course
- Neuromodulatory medications — amitriptyline, gabapentin, pregabalin at low doses
- Pelvic floor physiotherapy — surprisingly effective in some patients
- Nerve blocks — ilioinguinal, genitofemoral, pudendal blocks
- Cord denervation — surgical division of nerves around the spermatic cord, reserved for refractory cases
- Psychological support — chronic pain has a mental health dimension that benefits from acknowledgement
- Lifestyle adjustments — supportive underwear, activity modification, stress management
Emergency-ready.
Diagnostic-led.
Patient-centred.
Same-day acute evaluation
Acute testicular pain is triaged immediately. Same-day examination, immediate ultrasound, and emergency theatre access if torsion is suspected.
On-site Doppler ultrasound
Scrotal Doppler ultrasound at the clinic — no waiting for radiology referral. Quick definitive answer about blood flow, masses, infection.
Chronic pain taken seriously
When imaging is normal but pain persists, we don't dismiss — we work through a structured multimodal approach including medications, blocks, and physiotherapy.
Surgical capability when needed
Varicocelectomy, epididymectomy, cord denervation, hernia repair — surgical solutions are available under one roof, performed by the same surgeon.
Pricing for testicular
pain evaluation.
| Service | Starting from |
|---|---|
| Emergency consultation | ₹ [____] |
| Scrotal Doppler ultrasound | from ₹ [____] |
| Urine + STI screen | from ₹ [____] |
| Emergency scrotal exploration (suspected torsion) | from ₹ [____] |
| Bilateral orchidopexy | from ₹ [____] |
| Treatment for epididymo-orchitis (full course) | from ₹ [____] |
| Microsurgical cord denervation (refractory chronic pain) | from ₹ [____] |
Emergency and surgical care covered.
Emergency surgery for testicular torsion and other surgical interventions are covered by all major Indian insurers. We handle pre-authorisation. OPD evaluations may be partially covered or self-pay depending on policy.
Testicular pain —
your questions.
Torsion features: sudden onset (minutes), severe one-sided pain often with nausea/vomiting, the affected testicle may sit higher than the other. If you have any concern of torsion, treat it as an emergency — don't try to self-diagnose. Call us or go to ER.
Not necessarily. Intermittent severe pain can be intermittent torsion — the testicle twisting and untwisting. Anyone with recurrent episodes of severe one-sided testicular pain warrants urgent evaluation and often prophylactic orchidopexy.
Stress alone rarely causes new severe pain, but it can amplify existing chronic pain and contribute to chronic scrotal pain syndrome. Stress management is part of the multimodal approach to chronic pain.
Most testicular cancers are painless lumps. A minority (10–20%) present with pain or discomfort. Any new persistent testicular pain warrants ultrasound — partly to exclude this.
Brief discomfort after vigorous exercise can be normal. Persistent pain, swelling, or new bulges warrant evaluation. Exercise can also aggravate varicoceles, causing dragging pain — which is treatable.
Chronic scrotal pain syndrome — pain without identifiable structural cause — is real. Treatment is multimodal: anti-inflammatories, neuromodulatory medications (amitriptyline, gabapentin), nerve blocks, pelvic floor physiotherapy, and in refractory cases cord denervation surgery. We don't dismiss normal-imaging chronic pain.
Yes. Private consultation, confidential records. Family members and employers are not informed without consent.
Emergency surgery and most surgical interventions are covered by all major Indian insurers. OPD investigation may be partially covered or self-pay. We discuss costs upfront.