What is
a varicocele?
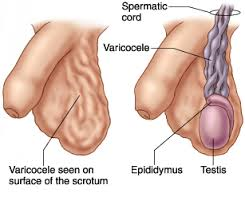
A varicocele is an abnormal enlargement of the veins that drain the testicle — a network called the pampiniform plexus. Essentially, it's varicose veins, but inside the scrotum. The valves in these veins fail, allowing blood to pool, the veins to dilate, and pressure to build.
The most important consequence isn't the appearance — it's the temperature effect. The testicles sit outside the body for a reason: sperm production requires a temperature 2–3°C below core body temperature. The pampiniform plexus normally acts as a heat exchanger, cooling blood before it reaches the testicle. When the plexus dilates with varicocele, this cooling function fails. Scrotal temperature rises. Sperm production gradually deteriorates.
This is why varicocele matters even in men with no scrotal symptoms — it can silently damage sperm production over years. About 15% of all men have a varicocele. Among men presenting with infertility, that rises to about 40%. The temperature link explains both numbers.
Why most varicoceles
are left-sided.
About 85–90% of varicoceles occur on the left side. Around 10–15% are bilateral. Pure right-sided varicoceles are uncommon — and when found, warrant additional investigation.
The reason is anatomical. The left testicular vein drains into the left renal vein at a 90-degree angle, against gravity, and travels a longer course before reaching the inferior vena cava. The right testicular vein drains directly into the inferior vena cava at an acute angle — a more efficient drainage path. The left side is biomechanically disadvantaged from birth.
Three clinical grades.
Plus subclinical.
Varicoceles are graded based on examination findings:
- Subclinical — not detectable on examination, seen only on Doppler ultrasound. Controversial whether to treat in isolation.
- Grade 1 — palpable only during Valsalva manoeuvre (straining, coughing). Mild dilation.
- Grade 2 — palpable on standing examination, without Valsalva. Moderate.
- Grade 3 — visible through the scrotal skin without examination. Classic "bag of worms" appearance. Severe.
Higher grades correlate with more significant sperm parameter abnormalities, though the relationship isn't perfectly linear. A Grade 2 varicocele in a 28-year-old with severely abnormal semen analysis warrants surgery just as much as a Grade 3 with milder parameters.
When varicoceles
announce themselves.
Most varicoceles are completely asymptomatic. The ones that cause symptoms tend to present in characteristic ways:
- Dragging, aching, or heavy sensation in the scrotum — often worse after prolonged standing, at the end of the day, in hot weather, or after exercise. Relieved by lying down.
- Visible enlargement of the scrotum on one side
- "Bag of worms" feeling on self-examination, particularly when standing
- Testicular discomfort or pain on the affected side
- Discovery during infertility workup — most common presentation
- Smaller testicle on the affected side (testicular atrophy)
- Reduced sperm parameters on routine semen analysis
- Lowered testosterone in some cases — varicocele is associated with reduced Leydig cell function in some men
In adolescents and young adults, a varicocele may be found incidentally on a sports physical or routine examination. In these cases the decision to treat depends on testicular size discrepancy (>20% difference) and Doppler findings — not just the presence of the varicocele.
Examination
plus ultrasound.
Diagnosis is usually straightforward, combining examination with imaging.
- Physical examination — done in a warm room (cold causes scrotal contraction and can hide a varicocele). Patient examined standing, with and without Valsalva manoeuvre. The varicocele feels like a "bag of worms" or thickened cord above the testicle.
- Scrotal Doppler ultrasound — confirms diagnosis, grades severity, measures vein diameter, assesses reflux on Valsalva, measures testicular volume on both sides. Essential before any surgical decision.
- Semen analysis — two samples, properly collected. Establishes baseline before any treatment, helps decide who needs surgery.
- Hormonal panel — testosterone, FSH, LH. Particularly relevant if there's testicular atrophy or borderline parameters.
- Right-sided imaging — for isolated right-sided or new-onset varicoceles, CT or MRI of the retroperitoneum to exclude underlying pathology.
Not every varicocele
needs surgery.
Infertility with abnormal semen
A couple struggling to conceive, where the male has a clinically palpable varicocele and abnormal semen analysis. The single strongest indication for surgery.
Significant pain
Chronic scrotal discomfort or pain attributable to the varicocele, after excluding other causes and trying conservative measures (scrotal support, analgesia).
Testicular atrophy in adolescent
Affected testicle smaller than contralateral side by >20%. Surgery before adulthood prevents long-term damage and protects future fertility.
Low testosterone
Selected cases where varicocele appears to be contributing to clinically low testosterone — emerging evidence supports surgery in this scenario.
Asymptomatic varicocele
An incidentally-found varicocele in a man with normal fertility and no symptoms generally does not need surgery. Surveillance only.
Subclinical varicocele
Detected only on ultrasound, not on examination. Generally not treated in isolation — evidence base is weak for benefit.
Microsurgical subinguinal
varicocelectomy is the gold standard.
Several techniques exist for varicocele repair. Outcomes are not equivalent.
| Technique | Recurrence | Hydrocele risk | Arterial preservation |
|---|---|---|---|
| Microsurgical SubinguinalGold standard | < 2% | < 1% | Excellent |
| LaparoscopicMostly historical now | 5–15% | 5–10% | Limited |
| Open RetroperitonealOlder approach | 10–15% | 7–9% | Poor |
| Radiological EmbolisationBy interventional radiology | 4–11% | 0% | Not applicable |
Why microsurgical is the standard:
- Lowest recurrence rate — operating microscope allows identification of every dilated vein, including small collaterals that other techniques miss.
- Lowest hydrocele rate — careful preservation of lymphatic vessels prevents post-op fluid accumulation.
- Testicular artery preserved — microscope identifies the artery clearly, protecting it from injury. This matters for testicular function.
- Day-care procedure — done under spinal or general anaesthesia. Most patients go home the same day or after single overnight stay.
- Small incision — 3 cm subinguinal incision. Cosmetic outcome excellent.
- Bilateral repair in single setting — if both sides need surgery, done in same anaesthetic.
What to expect after surgery:
- Mild discomfort for 5–7 days, controlled with simple analgesia
- Return to desk work in 5–7 days
- Avoid gym, heavy lifting, cycling for 3–4 weeks
- Sexual activity from 2–3 weeks
- Repeat semen analysis at 3 months — first improvement visible
- Further improvement up to 6–9 months as sperm cycles regenerate
What microsurgical repair
actually achieves.
Outcomes vary by initial severity and other factors, but the published evidence is consistent:
- 60–70% of men show significant improvement in semen parameters after microsurgical varicocelectomy
- 40–60% of couples achieve natural pregnancy within 12–18 months (when other female factors are favourable)
- Sperm count, motility, and morphology typically all improve — count improves most
- Testosterone rises modestly in many patients, particularly those with pre-op borderline-low T
- Pain resolves in 80–90% of men operated for varicocele-related discomfort
- Testicular catch-up growth in adolescents operated for testicular atrophy — typically 80–90% reach normal size
Microsurgical technique.
Couples-aware.
Honest outcomes data.
Operating microscope used
Microsurgical subinguinal varicocelectomy with operating microscope — not loupes, not laparoscopy. The technique with the best outcomes.
Honest expectations
We tell you realistic outcomes upfront — 40–60% natural pregnancy, not "guaranteed fertility." Surgery is highly worthwhile but not magical.
Day-care surgery
Most patients home same day. Single-side or bilateral in the same setting. Returning to desk work in under a week.
Couples care
We coordinate with reproductive medicine partners when needed. No commission referrals. The right path for your specific situation, not ours.
Pricing for varicocele
treatment.
| Service | Starting from |
|---|---|
| Consultation | ₹ [____] |
| Scrotal Doppler ultrasound | from ₹ [____] |
| Semen analysis (per sample) | from ₹ [____] |
| Hormonal panel | from ₹ [____] |
| Microsurgical varicocelectomy (unilateral) | from ₹ [____] |
| Microsurgical varicocelectomy (bilateral) | from ₹ [____] |
| Post-op review + 3-month semen analysis | from ₹ [____] |
Surgery covered. Workup often self-pay.
Microsurgical varicocelectomy is generally covered by major Indian insurers when medically coded (pain, infertility workup, testicular atrophy). Diagnostic workup may be partially covered. We handle pre-authorisation and discuss costs transparently upfront.
Varicocele —
your questions.
Generally no. Asymptomatic varicoceles in men with normal semen analysis and no testicular atrophy do not need surgery. Surveillance with periodic examination is sufficient. If you develop symptoms or are trying for a child, the picture changes.
No — but the evidence is strong. About 60–70% of patients show improved semen parameters and 40–60% of couples achieve natural pregnancy within 12–18 months (when other female factors are favourable). Outcomes depend on initial parameters and partner factors.
With microsurgical technique, under 2%. With older approaches (laparoscopic, open retroperitoneal), recurrence rates of 5–15% are reported. Technique matters significantly.
About 90–120 minutes for unilateral, 150–180 minutes for bilateral. Done under spinal or general anaesthesia. Most patients discharged the same day.
Sperm take about 72 days to mature. Initial improvement is typically seen at the 3-month repeat semen analysis. Further improvement continues up to 6–9 months. We routinely repeat semen analysis at 3 and 6 months post-op.
A small 3 cm incision is made in the groin crease, typically heals to a thin line that fades over months. Cosmetic outcome is good — the incision is in a discreet location.
Yes — radiological embolisation is an alternative for selected patients. Done by interventional radiology, no incision. Recurrence rates are somewhat higher than microsurgical (4–11%). Useful when surgical access is difficult or patient prefers it.
Mild to moderate discomfort for 5–7 days, controlled with simple analgesia (paracetamol, occasionally short course of anti-inflammatories). Most patients describe it as "soreness" rather than pain. Severe pain is unusual.
With microsurgical technique, no — the testicular artery is carefully preserved. Testicular atrophy after microsurgical varicocelectomy is extremely rare. Older techniques without microscope had higher rates of complications.